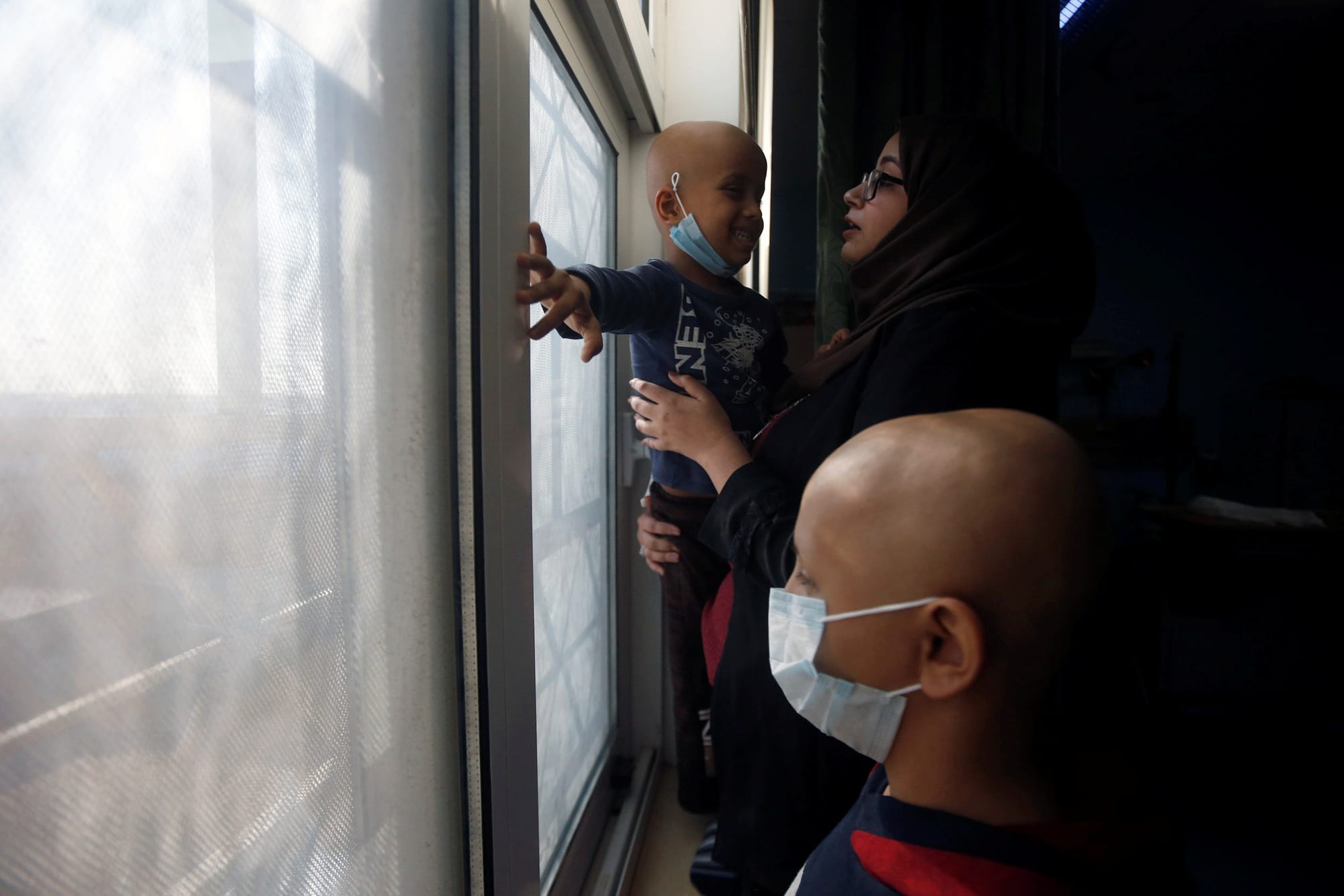
The Long Shadow of Iraq’s Cancer Epidemic and COVID-19
The epidemic of cancer in Iraq that emerged after the 1991 Gulf War has afflicted nearly every family. In response to a health care system devastated by sanctions and war, Iraqis acquired decades of experience piecing together novel mechanisms for obtaining treatment. The tendency of families to rel